Distal phalanx fractures are a common injury in both athletes and civilians. These fractures can differ greatly in severity and treatment indications depending on the size, location, and stability of the fracture in addition to appreciation of any bony comminution. Tendon avulsion in conjugation with a fracture complicates treatment and outcomes further. The classification system for these fractures have been well classified to include Type I, II, II, and IV with IV having subtypes. More recently, Type V has been added to the classification system. Designated as a comminuted distal phalanx fracture with flexor digitorum profundus avulsion, this Leddy-Packer type has two subgroups: namely, comminution without intra-articular involvement (Va) and comminution that includes the articular surface. We report the case of a 42-year-old female presenting with injury to the distal phalanx of the right small finger sustained after her dog ran away from her as she held the collar, exerting significant force in opposition to her flexed fingers. Upon exam and following appropriate imaging, her injury was defined as a Leddy and Packer Type Vb jersey finger injury. This was effectively treated with open reduction, internal fixation of the comminuted distal phalanx base and avulsion fragment. A notably rare injury, Leddy-Packer Type Vb distal phalanx avulsion injuries must be treated in a case-by-case basis, but open reduction internal fixation with plating proves an appropriate and effective means of repair in the correct patient.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Avulsion Fracture, Jersey Finger, Flexor Digitorum Profundus, Leddy-Packer Type Vb
1. Introduction
Distal phalanx fractures are a common injury in both athletes and civilians. These fractures can differ greatly in severity and treatment indications depending on the size, location, and stability of the fracture in addition to appreciation of any bony comminution. Tendon avulsion in conjugation with a fracture complicates treatment and outcomes further. Distal phalanx avulsion fractures, specifically of the flexor digitorum profundus tendon (FDP), are frequently seen in young athletes, often engaging in sports that involve tackling maneuvers, like football or rugby
[1]
Rizis D, Mahoney J. A rare presentation of flexor digitorum profundus type Vavulsion injury with associated intra-articular fracture: A case report. Can J Plast Surg. Summer 2011; 19(2): 62-3.
. Due to the common etiology, the term “Jersey Finger” is often used to characterize the injury. This presentation, however, is not only seen in the younger, active demographic, as the mechanism of injury includes any traumatic force hyperextending the distal interphalangeal (DIP) joint against contracted flexion
[4]
Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. The Journal of Hand Surgery. 1977/01/01/ 1977; 2(1): 66-69.
. Of note, it has been reported that over 75% of distal phalanx avulsion fractures occur in the ring finger due to its role in primary grip strength of the hand
[5]
Manske PR, Lesker PA. Avulsion of the ring finger flexor digitorum profundus tendon: an experimental study. Hand. 1978; (1): 52-55.
[6]
Murphy BA, Mass DP. Zone I flexor tendon injuries. Hand Clin. May 2005; 21(2): 167-71.
The classification system for these fractures has become well established but continues to evolve as unique presentations are documented. Jersey finger was first reported by von Zander
[4]
Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. The Journal of Hand Surgery. 1977/01/01/ 1977; 2(1): 66-69.
described three types of FDP tendon injuries in 1977 (Table 1). Type I is an FDP avulsion without fracture, with the tendon retracting into the palm and both vincula are ruptured
[4]
Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. The Journal of Hand Surgery. 1977/01/01/ 1977; 2(1): 66-69.
. Type II is the most common presentation with a small piece of bone becoming avulsed with the FDP tendon, leading to tendon retraction to the level of the proximal interphalangeal (PIP) joint. Type III presentations include a large bony fragment which does not retract proximal to the middle phalanx due to resistance created between the osseous fragment and the A4 pulley
[7]
Von Z. Trommlerlahmung Inaug. Dissertation, Berlin; 1891.
[7]
. Type IV injuries were included in the classification system following description by Smith
[9]
Smith JH. Avulsion of a profundus tendon with simultaneous intraarticular fracture of the distal phalanx—Case report. The Journal of Hand Surgery. 1981/11/01/1981; 6(6): 600-601.
in 1981. Type IV also include avulsion of a bony fragment, but the tendon is further avulsed from that fragment and retracted through flexor pulleys into the palm. Finally, Al-Qattan
[10]
Al-Qattan MM. Type 5 Avulsion of the Insertion of the Flexor Digitorum Profundus Tendon. The Journal of Hand Surgery: British; European Volume. 2001/10/01/ 2001; 26(5): 427-431.
described type V jersey finger most recently. Designated as a comminuted distal phalanx fracture with FDP avulsion, this Leddy-Packer type has two subgroups: namely, comminution without intra-articular involvement (Va) and comminution that includes the articular surface
[7]
Von Z. Trommlerlahmung Inaug. Dissertation, Berlin; 1891.
[8]
Stevens KA, Caruso JC, Fallahi AKM, Patiño JM. Flexor Tendon Lacerations. 2023 Feb 5. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 29630275.
[7, 8]
.
Table 1. Leddy and Packer classification system based on level of tendon retraction and presence of fracture.
Type
Description
Type I
FDP tendon retracted to palm
Type II
FDP retracts to level of PIP joint
Type III
Large avulsion fracture limits retraction to the level of the DIP joint
Type IV
Osseous fragment and simultaneous avulsion of the tendon from the fracture fragment (“Double Avulsion” associated with subsequent retraction of the tendon, usually into palm)
Type V
Ruptured tendon with bone avulsed and bony comminution of the remaining distal phalanx (Va, extraarticular, Vb, intra-articular)
In regards to treatment, it has been reported that early diagnosis and prompt surgical treatment lead to the best results
[4]
Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. The Journal of Hand Surgery. 1977/01/01/ 1977; 2(1): 66-69.
. However, these results are not consistent in practice and there is debate as to whether repair or nonoperative treatment yields the best results
[11]
Compton J, Wall LB, Romans S, Goldfarb CA. Outcomes of Acute Repair Versus Nonrepair of Zone I Flexor Digitorum Profundus Tendon Injuries. J Hand Surg Am. 2023 Aug; 48(8): 832. e1-832. e6.
Geary MB, Li KK, Chadderdon RC, Gaston RG. Complications Following Transosseous Repair of Zone I Flexor Tendon Injuries. J Hand Surg Am. 2020 Dec; 45(12): 1183. e1-1183. e7.
. Zone I flexor tendon injuries refer to injuries to the FDP tendon occurring over the proximal portion of the distal phalanx and distal to the flexor digitorum superficialis insertion
[6]
Murphy BA, Mass DP. Zone I flexor tendon injuries. Hand Clin. May 2005; 21(2): 167-71.
. Traditional methods for zone I FDP injuries include pull-out sutures, suture anchors, and transosseous repairs including K-wire fixation and in rare cases, plating
[8]
Stevens KA, Caruso JC, Fallahi AKM, Patiño JM. Flexor Tendon Lacerations. 2023 Feb 5. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 29630275.
[10]
Al-Qattan MM. Type 5 Avulsion of the Insertion of the Flexor Digitorum Profundus Tendon. The Journal of Hand Surgery: British; European Volume. 2001/10/01/ 2001; 26(5): 427-431.
Grant I, Pandya A, Mahaffey PJ. The Re-Attachment of Tendon and Ligament Avulsions. The Journal of Hand Surgery: British; European Volume. 2002/08/01/ 2002; 27(4): 337-341.
. Degree of articular involvement is the largest determinate in operative treatment approach in Leddy-Packer type Vb injuries. Overall, surgical intervention remains the mainstay for nearly all displaced distal phalanx FDP avulsion fractures.
2. Case Description
Presentation
The patient is a healthy 42-year-old right-handed female weighing 68 kg with a BMI of 20.22. She is a former “off and on” smoker since the age of 12, and she quit 1.8 years ago. She denies historical finger injury and presents to the emergency department with pain and swelling of the right small finger. She described the injurious event as she was firmly holding her dog’s collar when he abruptly pulled away, overcoming her grip while her finger stayed stuck in the collar. She felt immediate pain in the distal aspect of the finger that has not subsided since the event. There is notable swelling at the level of the DIP and distally. Her pain was controlled with analgesics, and a consult was placed with the hand surgeon.
3. Management
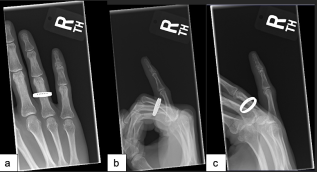
Upon three-view evaluation via x-ray and computer tomography (CT), the injury resulted in displaced fracture of the proximal aspect of the right fifth finger distal phalanx (Figure 1). The fracture extended into the articular surface without dislocation. Soft tissue edema was also noted. On physical examination, the patient experienced tenderness to palpation distal to the DIP joint of the right small finger. The finger remained neurovascularly intact, and the distal phalanx lacked active flexion upon exam. The patient elected to proceed with surgical treatment.
Figure 1. Fluoroscopic imaging (a) and lateral x-ray (b) taken upon presentation to the Emergency Department. X-rays are consistent with Leddy Packer Type Vb.
The patient underwent right small finger open reduction internal fixation (ORIF) of distal phalanx intraarticular fracture at the distal interphalangeal joint with repair of flexor digitorum profundus avulsion under local monitored anesthesia care (MAC) anesthesia.
The distal phalanx was exposed through a Bruner incision. A towel clip on the tip of the small finger was used by the physician assistant to help provide traction and manipulative the distal portion of the finger for aid in reduction. Once anatomic reduction of the articular surface was achieved, an OsteoMed plate was cut to the appropriate size and position. A 1-millimeter drill bit was used, and a total of four screws were used for fixation of the plate. To avoid nail bed damage, the distal screws were only 4-millimeters long. Two 8-millimeter screws were placed more proximally. Anatomic reduction of the fracture and plate position was confirmed with fluoroscopy (Figure 2). The patient followed up with hand therapy four days later for splint fabrication and instruction on restrictions. Follow up x-rays were taken at 2 weeks, 6 weeks, and 12 weeks postoperatively.
Figure 2. Intraoperative fluoroscopic lateral image of the hardware placement on the right small finger distal phalanx.
During the postoperative period, the patient had difficulties with wound healing, and 5 weeks after ORIF was treated with a wound debridement and secondary closure. After this, the patient’s symptoms improved, and we pursued a removal of hardware 7 weeks after hardware placement. At the next office visit following the removal of hardware, the patient’s fracture continued to be delayed in healing. She then began to use a bone stimulator and used this for approximately 8 weeks. At 20 weeks post open reduction internal fixation (ORIF), she showed a well healed distal phalanx fracture (Figure 3).
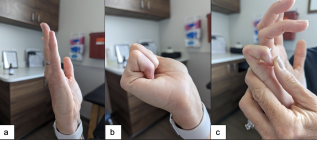
Figure 3. Patient’ range of motion at final Hand Therapy appointment showing full PIP motion (b and c) and full extension (a).
The patient had slightly decreased sensation over the ulnar side of the small finger and over her incision. Due to her sensitivity over the scar, we administered an intralesional corticosteroid injection. This injection significantly improved her symptoms. At the last office visit, the patient had full proximal interphalangeal (PIP) joint motion with 70 degrees of DIP flexion and full extension (Figure 4).
Figure 4. X-rays, AP (a), lateral (b), and oblique (c) views, show a healing distal phalanx fracture status post removal of hardware and 20 weeks post operatively.
4. Discussion
There has been much discussion regarding the classification system of distal phalanx avulsion fractures. Based upon the literature, specifically the more recent additions to the Leddy-Packer system by Al-Qattan
[10]
Al-Qattan MM. Type 5 Avulsion of the Insertion of the Flexor Digitorum Profundus Tendon. The Journal of Hand Surgery: British; European Volume. 2001/10/01/ 2001; 26(5): 427-431.
, the presented fracture falls under the description of a Leddy-Packer Type Vb. In review, the Type Vb fracture categorization includes tendon avulsion with an osseous fragment and concomitant fracture of the distal phalanx
[10]
Al-Qattan MM. Type 5 Avulsion of the Insertion of the Flexor Digitorum Profundus Tendon. The Journal of Hand Surgery: British; European Volume. 2001/10/01/ 2001; 26(5): 427-431.
. Type Vb is often more complex than the other types of jersey finger injury. Often, the distal and proximal fragments are minimally displaced, while the palmar fragments are markedly displaced due to FDP tendon forces
[9]
Smith JH. Avulsion of a profundus tendon with simultaneous intraarticular fracture of the distal phalanx—Case report. The Journal of Hand Surgery. 1981/11/01/1981; 6(6): 600-601.
. Unlike type IV injury, however, the volar fragment is attached to the FDP tendon, which has not retracted far into the palm as other categories have. Clearly, the fracture documented meets this criterion, as the base of the distal phalanx is notably comminuted with complete avulsion and a displaced palmar bony fragment.
Each of the Leddy-Packer types have differences in severity and unique treatment options. It is not difficult to achieve anatomical reduction, but achieving rigid fixation is challenging using strategies like pull-out sutures tied over a button on the dorsum of the finger 8. Regarding potential surgical intervention, the most complete indication for Type I and II fracture categorizations is FDP repair to the distal phalanx with either a pull through suture technique or with a suture anchor. Type III injuries require management of the fragment of bone as well, either with excision or fixation. Fixation can be difficult with a small fragment. Type IV requires fixation of the fragment first followed by repair of the tendon. Fixation of the fragment can be with a screw or K-wire, then the tendon repair is done similar to Type I and II injuries. Type V injuries become more complicated due to the comminution present. In order to get the best function of the DIP joint, anatomic reduction of the articular fragments is necessary. K-wires and screws are treatment options for stabilization of the fragments, but a plate offers more stable fixation by covering a broader area and distributing the compression forces of the screws over this area
[15]
Reformat DD, Nores GG, Lam G, et al. Outcome Analysis of Metacarpal and Phalangeal Fixation Techniques at Bellevue Hospital. Ann Plast Surg. Oct 2018; 81(4): 407-410.
. The downside to plate and screw fixation is more prominent hardware which may become symptomatic, leading to repeat surgery for hardware removal.
Albeit a primary concern, irritation from the plate must be monitored for sequalae in this region due to the minimal tissue. Overall, with significant comminution in conjugation with the displaced osseous fragment and avulsion, it was determined that ORIF with fixation via a plate and four screws has the best chance in yielding a great outcome for the patient.
5. Conclusion
In order to gain better understanding of the optimal treatment in unique distal phalanx fractures, it requires the dissemination of currently utilized modalities. By presenting and sharing cases like this one, the overall outcomes will improve as conversations within the hand-surgery community continue. The Leddy-Packer classification system is continuously evolving – thus, the treatment modalities are as well. It is our hope that the patient presented here can play a role in the evolution and education in Type Vb Leddy-Packer avulsion fracture management.
Statements
Informed consent was obtained, and sensitive patient medical information was not included. No funding was obtained any author. Procedures were in accordance with the ethical standards of human experimentation, and no animals were used in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Rizis D, Mahoney J. A rare presentation of flexor digitorum profundus type Vavulsion injury with associated intra-articular fracture: A case report. Can J Plast Surg. Summer 2011; 19(2): 62-3.
Von Z. Trommlerlahmung Inaug. Dissertation, Berlin; 1891.
[8]
Stevens KA, Caruso JC, Fallahi AKM, Patiño JM. Flexor Tendon Lacerations. 2023 Feb 5. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 29630275.
[9]
Smith JH. Avulsion of a profundus tendon with simultaneous intraarticular fracture of the distal phalanx—Case report. The Journal of Hand Surgery. 1981/11/01/1981; 6(6): 600-601.
Al-Qattan MM. Type 5 Avulsion of the Insertion of the Flexor Digitorum Profundus Tendon. The Journal of Hand Surgery: British; European Volume. 2001/10/01/ 2001; 26(5): 427-431.
Compton J, Wall LB, Romans S, Goldfarb CA. Outcomes of Acute Repair Versus Nonrepair of Zone I Flexor Digitorum Profundus Tendon Injuries. J Hand Surg Am. 2023 Aug; 48(8): 832. e1-832. e6.
Geary MB, Li KK, Chadderdon RC, Gaston RG. Complications Following Transosseous Repair of Zone I Flexor Tendon Injuries. J Hand Surg Am. 2020 Dec; 45(12): 1183. e1-1183. e7.
Grant I, Pandya A, Mahaffey PJ. The Re-Attachment of Tendon and Ligament Avulsions. The Journal of Hand Surgery: British; European Volume. 2002/08/01/ 2002; 27(4): 337-341.
Reformat DD, Nores GG, Lam G, et al. Outcome Analysis of Metacarpal and Phalangeal Fixation Techniques at Bellevue Hospital. Ann Plast Surg. Oct 2018; 81(4): 407-410.
Benjamin, W., Madeline, L., Patrick, J. (2024). Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report. International Journal of Medical Case Reports, 3(2), 13-17. https://doi.org/10.11648/j.ijmcr.20240302.11
Benjamin, W.; Madeline, L.; Patrick, J. Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report. Int. J. Med. Case Rep.2024, 3(2), 13-17. doi: 10.11648/j.ijmcr.20240302.11
Benjamin W, Madeline L, Patrick J. Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report. Int J Med Case Rep. 2024;3(2):13-17. doi: 10.11648/j.ijmcr.20240302.11
@article{10.11648/j.ijmcr.20240302.11,
author = {Wharton Benjamin and Labor Madeline and Johnston Patrick},
title = {Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report
},
journal = {International Journal of Medical Case Reports},
volume = {3},
number = {2},
pages = {13-17},
doi = {10.11648/j.ijmcr.20240302.11},
url = {https://doi.org/10.11648/j.ijmcr.20240302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20240302.11},
abstract = {Distal phalanx fractures are a common injury in both athletes and civilians. These fractures can differ greatly in severity and treatment indications depending on the size, location, and stability of the fracture in addition to appreciation of any bony comminution. Tendon avulsion in conjugation with a fracture complicates treatment and outcomes further. The classification system for these fractures have been well classified to include Type I, II, II, and IV with IV having subtypes. More recently, Type V has been added to the classification system. Designated as a comminuted distal phalanx fracture with flexor digitorum profundus avulsion, this Leddy-Packer type has two subgroups: namely, comminution without intra-articular involvement (Va) and comminution that includes the articular surface. We report the case of a 42-year-old female presenting with injury to the distal phalanx of the right small finger sustained after her dog ran away from her as she held the collar, exerting significant force in opposition to her flexed fingers. Upon exam and following appropriate imaging, her injury was defined as a Leddy and Packer Type Vb jersey finger injury. This was effectively treated with open reduction, internal fixation of the comminuted distal phalanx base and avulsion fragment. A notably rare injury, Leddy-Packer Type Vb distal phalanx avulsion injuries must be treated in a case-by-case basis, but open reduction internal fixation with plating proves an appropriate and effective means of repair in the correct patient.
},
year = {2024}
}
TY - JOUR
T1 - Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report
AU - Wharton Benjamin
AU - Labor Madeline
AU - Johnston Patrick
Y1 - 2024/08/15
PY - 2024
N1 - https://doi.org/10.11648/j.ijmcr.20240302.11
DO - 10.11648/j.ijmcr.20240302.11
T2 - International Journal of Medical Case Reports
JF - International Journal of Medical Case Reports
JO - International Journal of Medical Case Reports
SP - 13
EP - 17
PB - Science Publishing Group
SN - 2994-7049
UR - https://doi.org/10.11648/j.ijmcr.20240302.11
AB - Distal phalanx fractures are a common injury in both athletes and civilians. These fractures can differ greatly in severity and treatment indications depending on the size, location, and stability of the fracture in addition to appreciation of any bony comminution. Tendon avulsion in conjugation with a fracture complicates treatment and outcomes further. The classification system for these fractures have been well classified to include Type I, II, II, and IV with IV having subtypes. More recently, Type V has been added to the classification system. Designated as a comminuted distal phalanx fracture with flexor digitorum profundus avulsion, this Leddy-Packer type has two subgroups: namely, comminution without intra-articular involvement (Va) and comminution that includes the articular surface. We report the case of a 42-year-old female presenting with injury to the distal phalanx of the right small finger sustained after her dog ran away from her as she held the collar, exerting significant force in opposition to her flexed fingers. Upon exam and following appropriate imaging, her injury was defined as a Leddy and Packer Type Vb jersey finger injury. This was effectively treated with open reduction, internal fixation of the comminuted distal phalanx base and avulsion fragment. A notably rare injury, Leddy-Packer Type Vb distal phalanx avulsion injuries must be treated in a case-by-case basis, but open reduction internal fixation with plating proves an appropriate and effective means of repair in the correct patient.
VL - 3
IS - 2
ER -
Upper Extremity Surgery, Steamboat Orthopaedic and Spine Institute (SOSI), Steamboat Springs, USA; Department of Orthopedics, The University of Colorado School of Medicine, Aurora, USA
Upper Extremity Surgery, Steamboat Orthopaedic and Spine Institute (SOSI), Steamboat Springs, USA; Department of Orthopedics, The University of Colorado School of Medicine, Aurora, USA
Benjamin, W., Madeline, L., Patrick, J. (2024). Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report. International Journal of Medical Case Reports, 3(2), 13-17. https://doi.org/10.11648/j.ijmcr.20240302.11
Benjamin, W.; Madeline, L.; Patrick, J. Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report. Int. J. Med. Case Rep.2024, 3(2), 13-17. doi: 10.11648/j.ijmcr.20240302.11
Benjamin W, Madeline L, Patrick J. Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report. Int J Med Case Rep. 2024;3(2):13-17. doi: 10.11648/j.ijmcr.20240302.11
@article{10.11648/j.ijmcr.20240302.11,
author = {Wharton Benjamin and Labor Madeline and Johnston Patrick},
title = {Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report
},
journal = {International Journal of Medical Case Reports},
volume = {3},
number = {2},
pages = {13-17},
doi = {10.11648/j.ijmcr.20240302.11},
url = {https://doi.org/10.11648/j.ijmcr.20240302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20240302.11},
abstract = {Distal phalanx fractures are a common injury in both athletes and civilians. These fractures can differ greatly in severity and treatment indications depending on the size, location, and stability of the fracture in addition to appreciation of any bony comminution. Tendon avulsion in conjugation with a fracture complicates treatment and outcomes further. The classification system for these fractures have been well classified to include Type I, II, II, and IV with IV having subtypes. More recently, Type V has been added to the classification system. Designated as a comminuted distal phalanx fracture with flexor digitorum profundus avulsion, this Leddy-Packer type has two subgroups: namely, comminution without intra-articular involvement (Va) and comminution that includes the articular surface. We report the case of a 42-year-old female presenting with injury to the distal phalanx of the right small finger sustained after her dog ran away from her as she held the collar, exerting significant force in opposition to her flexed fingers. Upon exam and following appropriate imaging, her injury was defined as a Leddy and Packer Type Vb jersey finger injury. This was effectively treated with open reduction, internal fixation of the comminuted distal phalanx base and avulsion fragment. A notably rare injury, Leddy-Packer Type Vb distal phalanx avulsion injuries must be treated in a case-by-case basis, but open reduction internal fixation with plating proves an appropriate and effective means of repair in the correct patient.
},
year = {2024}
}
TY - JOUR
T1 - Management of Distal Phalanx Intraarticular Comminuted Fracture of Small Finger with Zone I Flexor Tendon Avulsion: A Case Report
AU - Wharton Benjamin
AU - Labor Madeline
AU - Johnston Patrick
Y1 - 2024/08/15
PY - 2024
N1 - https://doi.org/10.11648/j.ijmcr.20240302.11
DO - 10.11648/j.ijmcr.20240302.11
T2 - International Journal of Medical Case Reports
JF - International Journal of Medical Case Reports
JO - International Journal of Medical Case Reports
SP - 13
EP - 17
PB - Science Publishing Group
SN - 2994-7049
UR - https://doi.org/10.11648/j.ijmcr.20240302.11
AB - Distal phalanx fractures are a common injury in both athletes and civilians. These fractures can differ greatly in severity and treatment indications depending on the size, location, and stability of the fracture in addition to appreciation of any bony comminution. Tendon avulsion in conjugation with a fracture complicates treatment and outcomes further. The classification system for these fractures have been well classified to include Type I, II, II, and IV with IV having subtypes. More recently, Type V has been added to the classification system. Designated as a comminuted distal phalanx fracture with flexor digitorum profundus avulsion, this Leddy-Packer type has two subgroups: namely, comminution without intra-articular involvement (Va) and comminution that includes the articular surface. We report the case of a 42-year-old female presenting with injury to the distal phalanx of the right small finger sustained after her dog ran away from her as she held the collar, exerting significant force in opposition to her flexed fingers. Upon exam and following appropriate imaging, her injury was defined as a Leddy and Packer Type Vb jersey finger injury. This was effectively treated with open reduction, internal fixation of the comminuted distal phalanx base and avulsion fragment. A notably rare injury, Leddy-Packer Type Vb distal phalanx avulsion injuries must be treated in a case-by-case basis, but open reduction internal fixation with plating proves an appropriate and effective means of repair in the correct patient.
VL - 3
IS - 2
ER -